Long term results of high dose vancomycin loaded spacers for treating infected massive prostheses
Poster spacer ciment athenes 2019-2 Delepine F, Alkhallaf S. Delepine G.
Aim
infection is of the most devastating complication of conservative surgery using massive prosthesis, leading frequently to amputation. The aim of this bi centric study is to precise the influence of spacer loaded with high doses of vancomycin on late results
Patients From 1984 to 2010, we operated more than 670 patients with bone sarcoma. Aged 4,5 to 82 years (mean 25 y). Histology was osteosarcoma (330), Ewing (175), chondrosarcomas (148), fibrosarcomas or MFH (23), giant cell tumours in others. In 502 cases, p received chemotherapy, and radiotherapy in 50 cases. The median follow-up from tumour removal is 20.5 years. 62 p suffered of deep infection of the material used to reconstruct the skeletal defect. 3 p were refered to us for recurrence of deep infection initially treated elsewhere. Altogether, we treated 65 patients for deep infections.
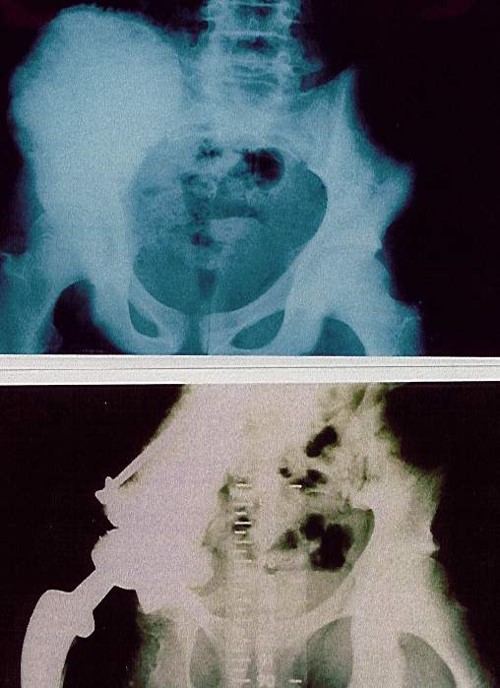
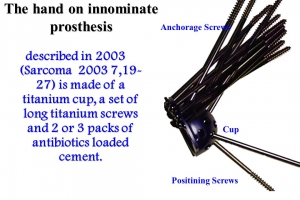
Method 28 p had debridment and cleaning of the prosthesis and long adapted antibiotherapy as first treatment. When ineffective (25/28), a removal of the prosthesis was performed with immediate re insertion of prosthesis in 19 cases. When infection recurred (16/19) and in 34 other patients the treatment included a two stages protocol with interposition of a spacer with antibiotic loaded cement during 4 to12 weeks .Until 2004, the spacer was made with gentamycin containing palacos mixed with conventional doses of antibiotics adapted to the germ. From 2004/6 we used high doses of vancomycin (4 g per batch of 40 g) with an average total dose of 11g of vancomycin per spacer. The new prosthesis was replaced secondarly when infection, cutaneous and muscular problems were solved.
RESULTS : At last control, 16 were amputated, following a mean of 6 ineffective procedures. 46 p. benefited from conservation surgery but a new prosthesis could be inserted only in 43, following a mean of 3.2 surgical procedures. Analysis shows the very bad prognostic value of initial radiotherapy, of distal locations, the importance of muscular coverage and the efficacy of high dose vancomycin in spacer. Up to date, none of the high dose vancomycin loaded spacers was followed by amputation
CONCLUSION Infection of massive prostheses is the most serious orthopaedic complication of limb salvage. Treatment must be preventive, avoiding any radiotherapy. Good prognostic factors of deep infection are early removal of the prosthesis, improvement of the muscular coverage, and use of spacers with high dose vancomycin.