Gardasil for boys: a too risky and too expensive bet!
by Gerard Delepine MD, oncologist surgeon gerard.delepine@bbox.fr
Would “HPV cancer of the anal canal” justify vaccinating the whole male population?
Pub is spreading fear in homosexual males and on all continents, to enlarge the market!
The French newspaper Le Monde published in May 2018 a forum[1]using fear, pain and misfortune, to promote vaccination against HPV in boys and prepare the population to the vaccinal obligation that demand the pharmaceutical lobby and its political and medical agents.
They want to extend to boys the recommendation of Gardasil, and add its obligation, to the mandatory 11 vaccines billed last year in France. This tribune of Le Monde was not written to inform on the 60 deaths registered each year in French males from cancer of the anus, but to prepare the population for a new obligation that would obviously be proposed for “equality between men and women, homo and heterosexual” (and the profit of the stock market?) In France, when a vaccine is mandatory, is no longer the guilty to compensate the victims but, the National Solidarity (our taxes). Mandatory vaccinations are worth!
Faith in a vaccine, coupled with greed does not justify the manipulation of facts. Recall the scientific data established by citing our sources, so that everyone can check.
IS IT REASONABLE TO IMPOSE TO ALL MALES A VACCINE AT RISK FOR A VERY MARGINAL PATHOLOGY THAT KILL SO FEW? [2]
What about the real danger of anal cancer?
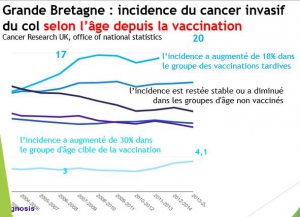
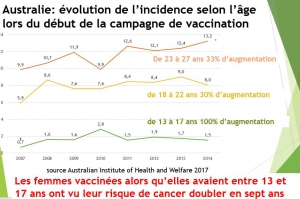
According to the different international cancer registries, the incidence[3] [4]of anal cancer has not been multiplied « by at least three in thirty years’ as claimed by the authors of this forum.
During the last three decades, the standardized incidence of anal cancer has increased in some countries by an average of 80 %, (in very close relation with the evolution of sexual practices.
40% in Norway (from 0.8 in 1985 to 1.1 in 2015 [5], 50% in the USA (from 1.2 in 1985 to 1.9 in 2015) [6], 63% in Great Britain (from 1.4 in 1995 to 2.4 in 2015)[7] , 100% in Denmark (0.68 to 1.48 for women and 0.45 to 0.80 for men between 1978 and 2008) [8], 90% in Australia (from 0.8 in 1982 to 1.5 in 2016) [9] , 84% in the Netherlands (0.45 in 1989 versus 0.83 in 2010) [10], 100% in France (from 0.2 to 0.5 for men and to 1.3 for women from 1982 to 2012) [11], 60% in Italy between 1983 and 2007 (1 to 2 for men and 1.8 to 2.5 for women) [12].
In contrast, no significant increase in incidence was observed in Spain, Israel, India, Japan, Singapore.
In countries where an increased incidence was observed, it is LINKED TO TWO HIGH RISK SUBGROUPS: IMMUNODEFICIENT AND PERSONS PRACTICING PASSIVE ANAL SEX.
PEOPLE TAKING IMMUNODEPRESSANT TREATMENTS suffer from an incidence of anal cancer 5 times higher than the overall population [13], rate close to that of heterosexuals infected with the AIDS virus [14] [15].
The practice of passive anal sex is the most important etiologic factor [16] [17] [18] [19] and partly explains the constant over risk of women compared to heterosexual men (1.5/100,000 to 3/100,000), and the risk 60 to 90 times higher of passive homosexual men (incidence 95/100,000) culminating at 130/100,000 among those who are carriers of the HIV virus[20].
The French authorities want to impose a generalized risky vaccination officially to protect a marginal population, «without stigmatizing it”. Given the small number of subjects at risk, the commercial interest (to double the sales!) probably justifies this apparent » kindness « , for these small groups?
ANAL CANAL CANCER, NOT A PUBLIC HEALTH PROBLEM
Except in these two high risk groups, anal canal cancer in men is not a public health problem. In France, it accounts for less than one-thousandth of all cancers, with around 280 cases reported among men and fewer than 60 deaths in 2015[21]. In USA it accounts for less than 0.5% of new cancers and 0.2% of all cancer deaths [22].
How to justify running the risks of an experimental vaccine to the entire population under these conditions?
As for cervical cancer, the merchants brandish the presence of HPV (cause or association?) to promote vaccination. Vaccine promoters affirm the causal link between papillomavirus infection and anal cancer, citing the actual statistical association between this infection and cancer. But association, concomitance do not necessarily mean causation, as we have pointed out in the case of cervical cancer.
FACTORS ASSOCIATED WITH ANAL CANCER
Those who are interested in anal canal cancer should consider known other associated factors likely to favour its occurrence sexually transmitted infections, smoking [23] [24] [25] [26] [27], number of partners.
All these factors are interrelated, and the establishment of causal link can only be based on the multifactorial analysis of the data of a large population, analysis never seriously made to our knowledge.
Given the extreme frequency of HPV infections in sexually active people and their spontaneous clearance in non-immunodeficient subjects, they could just as well represent a marker of sexual activity, likely as repeated microtrauma and other sexually transmitted infections to maintain chronic local inflammation whose carcinogenic role has been known for a long time.
PREVENTION OF ANAL CANCER
The reminder of these risk factors is necessary to lay the foundations for prevention that cannot be limited to promoting vaccines that have not yet proven effectiveness in preventing cancer.
Classic and effective primary prevention of the anal canal
The consensus basis of prevention of anal cancer includes using the condom for all intercourse, vaginal, oral or anal. Do not smoke and avoid exposure to tobacco smoke. And if you take drugs, always use single-use syringes. Avoiding contamination by HIV and other sexually transmitted diseases, certainly reduces the risk of developing anal cancer.
High risk for an experimental vaccine whose anti-cancer efficacy is not proven
To vaccinate all the young French, hoping thus to protect sexual minorities represents a too risky and too expensive bet. Even if the vaccine was effective, how much could it save from life from 60 annual deaths from this cancer? With what side effects on millions of French? At a prohibitive cost (around € 300 million euros /year) making this vaccine not cost effective in a country that can no longer afford a decent welcome in emergencies, or in the EPHAD (elderly hospitals) for which the minister, having “no magic, money “promised only 60 million € per year?
And for a very uncertain and even possibly negative medical benefit! Gardasil for boys? No thanks!
[1] Collective: In less than 30 years, the incidence of anal cancer has increased by at least three in most Western countries. Le Monde (Paris) May 2018
[2] Less than 60 deaths a year in France
[3] The incidence is the number of new cases that are observed per 100,000 people per year (Crude Rate)
[4] Since the cancer is more common in older people, the crude incidence is generally higher in a region where the elderly is more numerous. To avoid this bias, it is customary to normalize the crude incidence by the age structure of the population giving the standardized incidence. If the European or world standard population is used, the European standardized rate is obtained (European Standardized Rate or ESR), or World Standardized Rate (WSR)
[5] BT Hansen, S Campbell, Nygård M Long-term incidence of HPV related cancers, and cases preventable by HPV vaccination: a registry-based study in Norway
BMJ Open 2018; 8: bmjopen-2017-019005
[6] Surveillance Epidemiology and End Results (SEER) 13 Cancer Statistics Review, 1975-201
[7] Incidence of anal cancer; Cancer Research UK 2017
[8] Nielsen, Munk C, Kjaer SK Trends in the incidence of anal cancer and high-grade anal intraepithelial neoplasia in Denmark, 1978-2008. Int J Cancer. 2012 Mar1; 130 (5): 1168-73. 10.1002 / ijc.26115. Epub 2011 May 30
[9] Cancer in Australia 2017, page 81 can be downloaded http://www.aihw.gov.au/cancer-publications
[10] ARC Handbooks of Cancer Prevention Vol. 10: Cervix Cancer Screening. IARC Press. Lyon
[11] Bouvier AM1, Belot A, Manfredi S, Jooste V, Uhry Z, Faivre J, Duport N, Grabar S; French network of cancer registries FRANCIM. Trends of incidence and survival in squamous-cell carcinoma of the anal canal in France: a population-based study. Eur J Cancer Prev. 2016 May; 25 (3): 182-7
[12] Ferlay J, Bray F, Steliarova-Foucher E and Forman D. Cancer Incidence in Five Continents, CI5plus: IARC Cancer Base No.9 [Internet]. Lyon, France: International Agency for Research on Cancer; 2014. http://ci5.iarc.fr
[13] Grulich AE, van Leeuwen MT, Falster MO, et al. Incidence of cancers in people with HIV / AIDS compared with immunosuppressed transplant recipients: a meta-analysis. Lancet 2007; 370 (9581): 59-67.
[14] A. Nyitray MS Anal cancer and human papillomaviruses in heterosexual men Current oncology-volume 15, number 5 3 updates and developments in oncology 2008
[15] Grabar S, Moing V, Goujard C, et al. Clinical outcome of patients with HIV-1 infection according to immunologic and virologic response after 6 months of highly active antiretroviral therapy. Ann Intern Med 2000; 133: 401-10.
[16] Daling JR, Weiss NS, Hislop TG, Maden C, RJ Coates, Sherman KJ, et al. Sexual practices, sexually transmitted diseases, and the incidence of anal cancer. N Engl J Med 1987; 317 (16): 973-7
[17] Holly EA, Whittemore AS, Aston DA, Ahn DK, Nickoloff BJ, Kristiansen JJ. Anal cancer incidence: genital warts, anal fissure fistula gold, hemorrhoids, and smoking.
J Natl Cancer Inst 1989; 81 (22): 1726-31.
[18] Frisch M, Glimelius B, van den Brule AJ, Wohlfahrt J, Meijer CJ, Walboomers JM, et al. Sexually transmitted infection as a cause of anal cancer. N Engl J Med 1997; 337 (19): 1350-8
[19] Tseng HF, Morgenstern H, Mack TM, Peters RK. Risk factors for anal cancer: results of a population-based case-control study. Cancer Causes Control 2003; 14 (9): 837-46
[20]Silverberg MJ, Lau B, AC Justice, Engels E, Gill MJ, Goedert JJ, et al. Risk of anal cancer in HIV-infected and HIV-uninfected individuals North America. Clin Infect Dis 2012; 54 (7): 1026-34
[21]French High Council for Public Health Opinion on vaccination recommendations against human papillomavirus infections in men February 19, 2016
[22] Statistics at a Glance https://seer.cancer.gov/statfacts/html/anus.html
[23] Daling JR, Sherman KJ, Hislop TG, Maden C, Mandelson MT, Beckmann AM, Weiss NS. Tuxedo cigarette and the risk of anogenital cancer. Am J Epidemiol. 1992 Jan. 15; 135 (2): 180-9.
[24] Nordenvall C, Nilsson PJ, Ye W, Nyrén O. Smoking, snus use and risk of right- and left-sided colon, rectal and anal cancer: a 37-year follow-up study. Int J Cancer. 2011 Jan 1; 128 (1): 157-65.
[25] Coffey K, Beral V, Green J, Reeves G, Barnes I; Million Women Study Collaborators.
Br J Cancer.Lifestyle and reproductive risk factors. 2015 Apr 28; 112(9): 1568-74. Epub 2015 Mar 12.
[26] Daling JR, Madeleine MM, LG Johnson, and Human Papillomavirus alum, smoking, and sexual practices in the aetiology of anal cancer. Cancer. 2004 Jul 15; 101 (2): 270-80
[27] Holly EA, Whittemore AS, Aston DA, et al Anal cancer incidence: genital warts, anal fissure fistula gold, hemorrhoids, and smoking. J Natl Cancer Inst. 1989 Nov 15; 81 (22): 1726-31