par le Docteur G Delépine

Vouloir connaître l’avenir, un rêve dangereux
L’homme a besoin de sécurité. Pour s’exonérer des inquiétudes liées aux vicissitudes de la vie. Il aime se rassurer avec des prédictions. Mais croire en celles-ci peut entraîner des conséquences funestes.
Crésus, voulant savoir si la guerre contre l’Empire perse lui serait favorable, alla consulter l’oracle de Delphes. La Pythie lui prédit « si tu fais la guerre, un grand empire s’effondrera ». Il fit la guerre et son empire s’effondra.
Avant de déclarer la guerre contre le Covid-19, Macron consulta l’oracle de l’Imperial College de Londres qui prédit :
« si tu ne fais rien, tu pourrais déplorer 500 000 morts en France ».
Macron le crut, mit la population française en résidence surveillée et fit de la France l’un des pays d’Europe occidentale où la mortalité du Covid19 est l’une des plus élevées.
Au 9 janvier 2021, les 5 grands pays européens qui ont confiné à l’aveugle se retrouvent dans le top 5 européen de la mortalité par million d’habitants avec une mortalité de 2531/M en Belgique, 2383/M en Italie, 1967/M en Espagne, et 1914/M en France.

Contrairement aux prédictions de Ferguson, le confinement aveugle a été suivi d’une mortalité Covid 19 accrue.
Simulations et prophéties
Les confinements et les mesures liberticides qu’on nous a imposés ne reposent sur aucun fait scientifique constaté dans le monde réel, mais uniquement sur la terreur inspirée par la prophétie apocalyptique de Ferguson, simple simulation mathématique basée sur des hypothèses fausses.
Cette Pythie britannique a remplacé le dieu Apollon par un ordinateur et tire ses prédictions de simulations numériques, utilisant des programmes informatiques modélisant un phénomène dont ils peuvent à volonté modifier les constantes de base.
Les modélisations se sont révélées très fécondes dans les sciences dures (physique, chimie, mathématiques) dont les lois sont immuables. Mais l’HOMME n’est pas un objet comme les autres.
Appliquées sans discernement à des phénomènes biologiques et/ou reposant sur des hypothèses incertaines, ces prédictions ne valent guère mieux que celles de Nostradamus. Leur danger particulier est qu’auréolées de l’aspect scientifique de l’informatique, des statistiques et modélisations soient considérées comme fiables et utilisées par des politiques crédules soumis au mythe de la technique, pour décider une action dans le monde réel, et particulièrement dans le domaine médical.[1]
Les êtres vivants, tous différents, tous uniques, sont beaucoup plus complexes que des entités mathématiques et s’adaptent aux menaces. Croire que les humains se conforment toujours aux prévisions issues d’algorithmes et de scénarisations de données revient à nier leur humanité. C’est en cela que la médecine diffère largement des sciences exactes et qu’elle périclite, depuis qu’elle est dirigée par des chercheurs se prétendant scientifiques et non plus par des docteurs au chevet des malades.
Les lourds antécédents de Ferguson auraient dû alerter
Ferguson avait prédit que la grippe H1N1 serait une pandémie meurtrière et que seul le vaccin pourrait éviter l’hécatombe. Au Canada il avait prédit 8000 morts et en France plus de 20 000. Au Canada il y en a eu moins de 500 et en France 312.
Ses prédictions catastrophiques et la campagne de propagande de R Bachelot nous ont coûté plus de 2 milliards d’euros en achat de vaccins et de Tamiflu et causé de trop nombreuses victimes de la vaccination inutile.
En 2001, ses prédictions sur la fièvre aphteuse ont entraîné l’abattage de 6 millions de bovins, décision aujourd’hui considérée comme aberrante et qui a coûté environ 6 milliards de livres aux éleveurs anglais.
En 2002, le prophète Ferguson affirma que la maladie de la vache folle tuerait environ 50 000 Britanniques. À la fin de l’épidémie, on en recensa 177.
En 2005, il prédit que la grippe aviaire tuerait 65 000 Britanniques. Il y en eut au total 457.
Sa surestimation considérable des risques a concerné aussi l’Ebola.
Les erreurs grossières des simulations de Ferguson sur les épidémies passées auraient dû inciter nos dirigeants à être plus circonspects, à ne pas croire aveuglément ce prophète de malheur et à ne surtout pas appliquer ses préconisations dont les conséquences sanitaires, sociales et économiques (qu’il n’a jamais prises en compte) ont été catastrophiques, même si nos gouvernants tentent de le cacher par de nouvelles simulations publicitaires réalisées à la demande par des élèves français de Ferguson.
Que des prédictions soient fausses n’a rien d’étonnant. Ce qui l’est davantage c’est d’une part l’importance des surestimations (10 à 20 fois supérieure à la réalité) et d’autre part leur caractère systématiquement pessimiste. Une erreur due au hasard aurait été tantôt trop pessimiste, tantôt trop optimiste. Statistiquement le caractère toujours catastrophique de ses prédictions ne peut pas être dû au hasard (p<0,02). Cette improbabilité statistique traduit-elle un modèle faux ou une volonté délibérée de tromper ses lecteurs pour les terroriser ?
La prophétie Covid totalement délirante de Ferguson[2]
Détaillée dans le rapport 9 de l’Imperial College[3] prophétisait, un pic de mortalité vers le 3e mois de l’épidémie, avec des hôpitaux bondés et des lits de soins intensifs saturés.
« Pour une épidémie non maîtrisée, nous prévoyons que la capacité en lits de soins intensifs sera dépassée dès la deuxième semaine d’avril, avec un pic de la demande en soins intensifs plus de 30 fois supérieur à l’offre maximale possible dans les deux pays et un nombre total de décès de 510 000 en Grande-Bretagne et de 2,2 millions aux USA, et cela sans tenir compte des morts supplémentaires liées à l’absence de traitement d’autres maladies du fait de la saturation des hôpitaux. »
Ce scénario de film d’horreurn’est pas de la science, mais au mieux de la science-fiction-film-catastrophe évoquant les prédictions de Nostradamus.
Par exemple, le rapport 9 estimait que sans confinement la Suède verrait ses hôpitaux débordés en quelques semaines et obligés de trier les malades. Il prévoyait 70 000 morts en 6 mois. Au 6 février 2022, sans confinement ni mesures autoritaires, les hôpitaux suédois n’ont jamais été débordés, et le nombre de morts a atteint 16 100, soit 4 fois moins que les prédictions de Ferguson, en quatre fois plus de temps. Et rappelons-le : sans masque, sans distanciation forcée, sans fermeture d’écoles, ni de restaurant ou de musée.
Fort de leur certitude quasi religieuse, N Ferguson et ses élèves ne sont même pas rigoureux.
Ainsi dans un article rédigé pour justifier a posteriori le bien-fondé des mesures sanitaires autoritaires, ils se vantent d’avoir sauvé 3 millions d’Européens grâce au confinement. Dans cet article, scandaleusement diffusé par Nature,[4] ils publient un tableau qui détaille pays par pays le « nombre de morts évitées par le confinement » et affirment avoir sauvé 560 000 Allemands et 26 000 Suédois grâce au confinement.
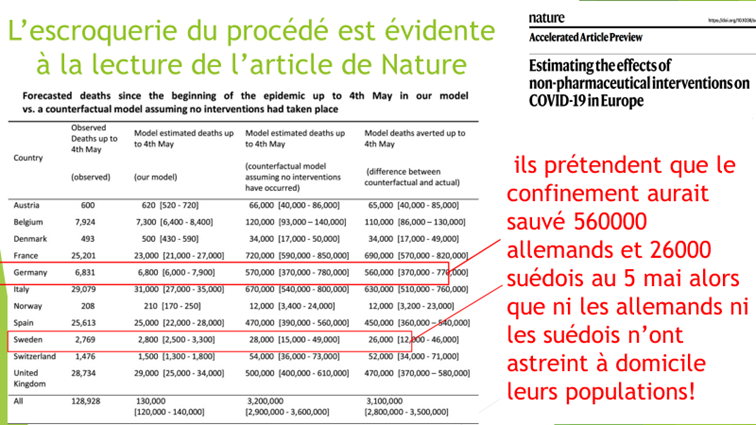
Mais les auteurs de cette escroquerie n’ont pas remarqué que ni les Suédois ni les Allemands n’avaient confiné !
Le 25 mars 2020, Neil Ferguson interrogé par la commission parlementaire britannique de la science et de la technologie a reconnu que sa première estimation était trop pessimiste et a ajouté « les deux tiers des gens qui mourront seraient de toute façon morts dans l’année ». Aveu tardif et exprimé sans remords.
Le gouvernement par la peur et le chantage aux libertés
Depuis le début de la crise, à chaque fois que la situation réelle s’améliore, les « enfermistes » inventent une nouvelle prophétie catastrophe pour raviver la peur et imposer de nouvelles restrictions des libertés.
Comme Veran sonnant l’alarme en fin juin 2021 :
« Une nouvelle vague de Covid dès la fin juillet » !
Arnaud Fontanet :
« À la rentrée, en septembre-octobre, on aura une nouvelle vague de cas » de Covid-19.
Jean-François Delfraissy :
« On doit se souvenir de ce qui s’est passé l’été dernier : on était à des chiffres à peu près comparables, et on a vu la deuxième vague en septembre ».
Comme l’Institut Pasteur :
« Sous des hypothèses réalistes concernant le R0 du variant dominant et la couverture vaccinale cet automne (2021), un pic d’hospitalisations important est possible en l’absence de toute mesure de contrôle de l’épidémie »
Car depuis le début de la crise les propagandistes de Big Pharma qui nous gouvernent ont compris que le moyen le plus efficace de contraindre la population à subir des injections expérimentales, inutiles et dangereuses est le chantage aux libertés « vous serez libres si vous vous vaccinez ».
Puis comme tous les maîtres chanteurs, dès que vous leur cédez, ils renient leur promesse (vaccinés, mais pas plus libres) et augmentent leurs exigences : une injection de plus, puis une autre et encore une autre…
Ce n’est pas pour rien que dans les séries policières les victimes des maîtres chanteurs se retrouvent souvent contraintes pour se libérer, de les assassiner.
Il n’y a plus de raison d’avoir peur
Depuis juin 2021 la mortalité quotidienne moyenne est de 100/J, soit environ 6 % de la mortalité globale.
Le pic Omicron a été atteint le 28 janvier 2022 et l’épidémie a déjà régressé de près de 50 %.

Une fois la vague Omicron passée, l’immunité naturelle protégera enfin la population, comme auraient dû le faire les injections anti-covid s’il s’agissait de vrais vaccins réellement testés.
D’ailleurs, la très grande majorité des agences sanitaires du monde entier appellent maintenant à traiter le covid comme une grippe ordinaire.
Il ne faut pas davantage avoir peur de la suppression des mesures sanitaires qui nous pourrissent la vie depuis deux ans.
Partout dans le monde les peuples se réveillent de l’hypnose qu’avaient suscitée ces prophéties catastrophes et les gouvernements, sous la pression, sont contraints de supprimer leurs mesures restrictives de liberté.
Continuons le combat pour accélérer le respect de nos droits fondamentaux.