« Turbo-cancer » est un terme de langage courant, populaire, non réellement scientifique, pour évoquer l’émergence récente de cancers très agressifs qui se développent très rapidement ». Il est apparu au cours de l’année 2021 après que l’injection covid 19 se soit répandue comme une trainée de poudre dans une majeure partie du monde occidental… Coïncidence ou causalité ?
Les premiers cancers post vaccination sont apparus très tôt
L’attention des médecins cliniciens – ceux qui voient de vrais malades en consultation, les interrogent et les examinent- avait été très tôt attirée par des modifications de l’évolution clinique de certains patients dans les quelques mois suivant les débuts de la campagne d’injections anticovid. Initialement ce furent des rechutes brutales, et résistantes, de patients apparemment guéris de cancer depuis plus de dix, quinze ans voire plus, en rémission complète, qui sidérèrent les généralistes et les cancérologues (qui ne l’avouèrent que sous le manteau…).
Un exemple typique a été celui de monsieur Axel Kahn, président de la ligue contre le cancer, qui s’était fait remarquer par ses positions extrémistes pro vaccins covid et dont le cancer d’évolution jusqu’ici lente a explosé après sa vaccination l’emportant en quelques mois.
De nombreuses malades en rémission de cancer du sein rechutèrent contre toute attente après une si longue durée.
Parallèlement les médecins virent arriver dans leurs cabinets de très jeunes gens d’une vingtaine d’années ou moins atteints de maladies hématologiques, telles des lymphomes, des glioblastomes etc. d’apparition jusqu’ici exceptionnelle chez les jeunes, d’évolution particulièrement rapide et résistant trop souvent à toute espèce de traitement.
Les témoignages se multiplient par mail, téléphone, rencontres, réseaux sociaux, groupes sur telegram etc.. Tel un voisin bien portant de 83 ans injecté qui meurt en deux mois d’un cancer du pancréas, cancer au premier rang des récits pris au hasard, peut-être parce que ce cancer est particulièrement difficile à traiter et rapidement mortel.
Un des autres cancers les plus rapportés dans nos contacts récents est le lymphome chez de jeunes adultes…
Et tous ces articles qui fusent et disparaissent rapidement sous l’effet de la censure féroce sur internet.
« En tant qu’oncologue, je vois des personnes atteintes d’un cancer stable [qui a] progressé rapidement après avoir été forcées de recevoir un rappel ».
En mars 2021, le Dr Ryan Cole a signalé une « hausse » massive de diverses maladies auto-immunes et cancers chez les patients vaccinés contre la COVID. « Depuis le 1er janvier 2021, en laboratoire, je constate une multiplication par 20 des cancers de l’endomètre par rapport à ce que je vois sur une base annuelle ».
Bref de quoi étonner les cancérologues qui ne firent que chuchoter au début, puis s’exprimèrent enfin entre eux. Pourquoi ce silence ? C’est un autre versant des conséquences psychiatriques de cette plandémie.
Camouflage et censure des faits, diffamation et menaces contre les donneurs d’alerte.
Etant donné la concomitance des campagnes d’injection, les médecins du monde entier constatèrent les mêmes phénomènes en même temps, rendant la coïncidence moins crédible que la causalité. Les prétendus « sites de vérification » des médias officiels (les fameux fact checkers largement rémunérés par Bill Gates entre autres ) s’empressèrent de nier toute possibilité d’une responsabilité des vaccins et certains collègues défenseurs du crédo officiel diffamèrent en les traitant de fous les lanceurs d’alerte , à commencer par Mme le Pr Alexandra Henrion- Caude qui expliquait ce qu’est l’ARNm dans son best -seller « les apprentis sorciers ».. )
Pour camoufler la triste réalité de la flambée des cancers post injection expérimentale, que la population commençait à découvrir seule, on vit fleurir des papiers sur l’augmentation de cancers depuis trente ans. Une étude publiée dans BMJ Oncology intitulée « Tendances mondiales de l’incidence, de la mort, du fardeau et des facteurs de risque du cancer précoce de 1990 à 2019 » a signalé une augmentation de 79,1% de l’incidence du cancer chez les personnes de moins de 50 ans au cours des trente dernières années . Mais une analyse objective du phénomène, aurait souligné les différences de pratique médicale sur ces décennies et tout particulièrement la pratique de dépistage à outrance des cancers du sein, de la prostate, du colon, de la thyroïde qui a conduit à traiter des patients dont le cancer n’aurait sans doute jamais évolué, contribuant ainsi à accroitre artificiellement le nombre réel de cancer, à en augmenter les taux de guérison apparents tout en administrant inutilement aux patients des traitements dangereux.
Au total plus de 350 organes de presse à travers le monde ont publié des articles rapportant les résultats des cancers avant 2019 et leur dramatique augmentation, alors qu’après trois ans de plandémie covid et des milliers de victimes des injections, le sujet est soigneusement évité dans les journaux mainstream, sauf récemment dans les quotidiens ou hebdomadaires allemands ou suisses, anglais, accompagnés parfois d’excuses aux lecteurs de ne les pas avoir informés plus tôt…
Rappels des faits publiés depuis la crise covid.
France
L’Institut du Cancer ne donne pas les chiffres de cancers des cinq dernières années, (depuis 2018) et en particulier les mortalités, prétextant qu’: « En raison d’un changement de méthode de codage d’enregistrement des cas, les données de mortalité actualisées ne sont pas disponibles. ».
Les données n’étant pas accessibles en France, on se réfèrera aux rares données publiées dans les pays anglophones.
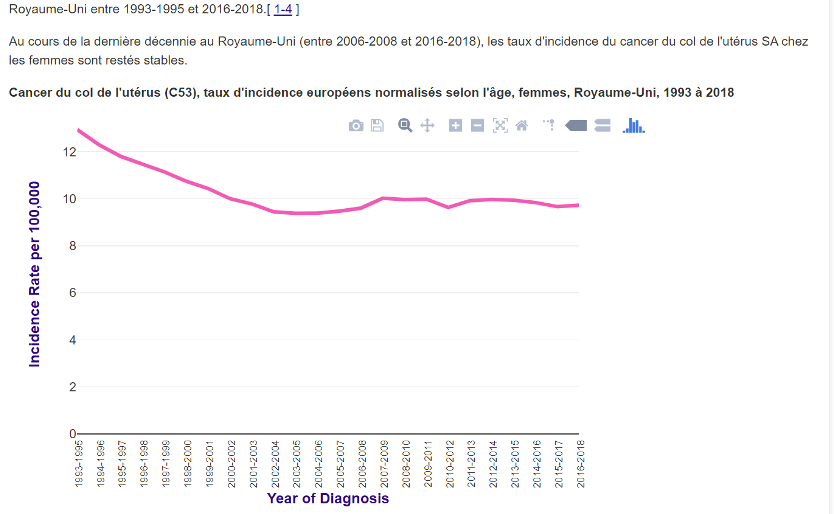
Royaume Uni.
Phinance Technologies, une société spécialisée dans l’exploration de données indépendantes et la consultation, a publié une analyse des demandes d’invalidité au Royaume-Uni au cours des sept dernières années (https://phinancetechnologies.com/HumanityProjects/PIP Analysis-Systems.htm). Ainsi, indirectement, via le biais des nouvelles invalidités, on peut déduire le nombre global de malades et celui par pathologies sur ces dernières années. Mieux que rien.
Après les injections de nombreuses personnes sont fatiguées, vont d’arrêt de travail en tentative de reprise, et nouvel arrêt et il ne s’agit pas uniquement de dépressions.
Le nombre total de nouvelles demandes de prestations d’autonomie personnelle (RRP) pour tous les âges et toutes les causes présentées par des personnes ayant présenté une demande d’invalidité a très fortement augmenté. En 2022 le taux de nouvelles demandes a été supérieur de 71% au taux moyen de 2016-2019 et a suivi le déploiement du vaccin Covid.
Si l’augmentation du nombre total de personnes demandant des prestations d’invalidité au Royaume-Uni parce qu’elles sont devenues incapables de travailler- se répète dans le monde entier, en 2022, il y aura eu 31 millions de nouveaux cas d’invalidité.
Un drame qui est peut être en partie responsable des soucis des petits patrons pour trouver du personnel.
Phinance Technologies rapporte également les données distinctes pour les paiements versés aux personnes souffrant d’invalidité en raison de l’incidence du cancer. Le nombre des bénéficiaires de ces paiements a augmenté de 35 % en 2022 par rapport à la moyenne à long terme. Une augmentation de 12 271 cas.
Il est triste de constater qu’une augmentation de 79% d’apparition de cancers sur une période de trente ans a suscité une forte inquiétude et une publicité mondiales, alors qu’une augmentation de 35% de l’incidence du cancer en à peine plus d’un an après le début du déploiement du vaccin, un taux annuel 13 fois plus élevé, a été ignorée par les médias grand public. Si cette augmentation était reproduite dans le monde entier, cela équivaudrait à 1 million de cas de cancer supplémentaires.
L’analyste de données Edward Dowd a fait la lumière sur les autorisations indemnisations annuelles au Royaume-Uni accordées pour invalidité en utilisant différentes mesures pour 2020, 2021 et 2022. Et ce qu’il a constaté, c’est que les demandes pour maladies hématologiques cancéreuses(leucémies) étaient en 2022 en hausse stupéfiante de 522% au-dessus de la tendance des années précédentes.
Nouvelle-Zélande.
L’enquête sur la population active auprès des ménages indique que 6600 personnes en âge de travailler (15-64 ans) ont quitté le marché du travail en raison d’un handicap au cours de l’année écoulée depuis juin 2021, date à laquelle la vaccination de ce groupe d’âge a commencé.
La fuite de données hospitalières de la région de Wellington a révélé une incidence croissante de cancers et en particulier des leucémies (+ 25%), des cancers du sein (+24%), des glioblastomes (+15%) et des cancers du pancréas (+15%).
Le financement continu par les gouvernements de « vérificateurs de faits » (fast checkers) qui se comportent en vrais experts en désinformation, niant les preuves scientifiques croissantes des dommages causés par les vaccins Covid, devient une affaire mondiale, non seulement morale mais politique, menaçant la science et la démocratie.
Aux USA
Le registre des déclarations des accidents vaccinaux VAERS a enregistré une hausse considérable (123%) des cancers survenus après vaccination covid lorsqu’on la compare aux années précédentes.
Cette augmentation des cancers post vaccinaux n’est pas due à une utilisation plus massive des vaccins covid par rapport aux autres vaccins; en effet durant les années précédentes qui servent de comparaison les vaccins anti grippaux ont été chaque année plus largement injectés que les vaccins covid en 2021.
En janvier 2022, trois militaires de haut rang, médecins responsables de la santé publique aux USA, ont déclaré sous serment qu’à la suite de l’adoption du vaccin COVID dans l’armée américaine ils avaient constaté une augmentation des cancers de 296 %4.
Causes possibles de ces turbo-cancers
Certains scientifiques cherchent absolument à comprendre ce qui se passe au fin fond de nos cellules agressées, car semble-t-il certains ont du mal à croire la simple observation clinique s’ils n’en comprennent pas le mécanisme (pourtant souvent mystérieux en médecine).
« En raison de la dérégulation des réponses immunitaires et de la suppression du système immunitaire par ces injections génétiques … ces cancers qui seraient normalement contrôlés par le corps se développent de manière inattendue très rapidement », a déclaré le Dr Ryan Cole dans une interview avec Children’s Health Defense.
Les protéines de pointe des vaccins à ARNm servent de carcinogène, nourrissant littéralement le cancer et le propulsant à se multiplier de manière exponentielle pour envahir le reste du corps. (ibid 1) Turner a également observé de plus en plus de tumeurs multiples dans plusieurs organes, ainsi que des récidives et des métastases incontrôlables ».
En ce qui concerne l’immunité adaptative globale, Cole décrit : « Après le vaccin, ce que nous voyons est une baisse des cellules T tueuses » qui « gardent tous les autres virus sous contrôle », laissant le patient vulnérable à une variété de maladies.
En octobre 2022, une étude suédoise a confirmé que la protéine de pointe associée à la maladie COVID-19 et ses vaccins expérimentaux pénètre dans le noyau des cellules et interfère de manière significative avec les fonctions de réparation des dommages à l’ADN, compromettant l’immunité adaptative d’une personne et facilitant peut-être la formation de cellules cancéreuses.
Un post de la généticienne Alexandra Henrion- Caude auteur des « les apprentis …) pour sensibiliser les humains au risque de cancer après injection anticovid pourra -t-il sauver des enfants et adolescents de ces injections catastrophiques ?
« Je remarque que l’humain comprend mieux sur l’animal que sur lui-même. Alors je vous raconte l’histoire de Kimani, le petit gorille, né dans un zoo à Calgary. Il est né le 9 mars 2016 d’une mère Kioja, âgée de 15 ans (primipare) et d’un père illustre Kakinga, connu comme le « gentle giant » (le gentil géant), mort à 37 ans d’une déchirure de l’aorte.
Bénéficiant du nec plus ultra du traitement de l’humanité, le jeune Kimani âgé de 6 ans a été injecté début avril 2022 avec les premières doses anti-COVID19 disponibles au zoo.
En moins de 2 mois, l’état de santé de Kimani s’est profondément dégradé. Il est dans un état critique, et seuls les soins palliatifs sont désormais envisagés. Il a été diagnostiqué d’un cancer du foie ».
Et une lettre du Dr Angus Dalgleish, professeur d’oncologie à l’Université St George de Londres, au Dr Kamran Abbasi, rédacteur en chef du BMJ pour que le BMJ fasse du consentement libre et éclairé préalable pour la vaccination Covid un sujet prioritaire.
« Cher Kamran Abbasi,
Covid n’a plus besoin d’un programme de vaccination étant donné que l’âge moyen de décès de Covid au Royaume-Uni est de 82 ans et alors que pour toutes les autres causes il est de 81 ans et en baisse.
La responsabilité des injections anti covid avec les caillots, la myocardite, les crises cardiaques et les accidents vasculaires cérébraux est maintenant bien acceptée, tout comme le lien avec la myélite et les neuropathies. (Nous avons prédit ces effets secondaires dans notre article de juin 2020 Sorensenet al. 2020, l’analyse de l’explosion ayant révélé 79% d’homologies avec les épitopes humains, en particulier PF4 et la myéline.)
Cependant, il y a maintenant une autre raison d’arrêter tous les programmes de vaccination. En tant qu’oncologue praticien, je vois des personnes atteintes d’une maladie stable progresser rapidement après avoir été forcées de prendre un rappel, généralement pour pouvoir voyager.
Même au sein de mes contacts personnels, je vois une maladie à base de cellules B après les rappels. Ils décrivent être nettement malades quelques jours à quelques semaines après le rappel – une leucémie en développement, deux collègues de travail lymphome non hodgkinien et un vieil ami qui a eu l’impression d’avoir eu le Covid long depuis qu’il a reçu son rappel et qui, après avoir eu une douleur osseuse intense, a été diagnostiqué comme ayant de multiples métastases d’une maladie rare des cellules B.
J’ai suffisamment d’expérience pour savoir que ce ne sont pas les anecdotes fortuites que beaucoup suggèrent, d’autant plus que le même schéma est observé en Allemagne, en Australie et aux États-Unis. Les rapports d’immunosuppression innée après ARNm pendant plusieurs semaines conviendraient, car tous ces patients à ce jour ont un mélanome ou des cancers à base de cellules B, qui sont très sensibles au contrôle immunitaire – et c’est avant les rapports de suppression du gène suppresseur par ARNm dans les expériences de laboratoire Cela doit être diffusé et débattu immédiatement ».
Angus Dalgleish
Les injections répétées de COVID conduisent des variantes dangereuses, et des cancers turbo
APPEL AU BON SENS
Selon le vaccinologue Geert Vanden Bossche, DVM, Ph.D., la poursuite de la vaccination de masse contre la COVID-19 suscite de nouvelles souches virales (les variants) plus infectieuses et potentiellement dangereuses, augmentant le risque de COVID-19 grave, tout en entraînant une augmentation de cancers agressifs et de maladies auto-immunes dans les populations vaccinées. Dans son article récent en cet été 23, Vanden Bossche envoie un «avertissement sévère à ceux qui envisagent de se faire vacciner contre la COVID-19 plus tard cette année, alors que nous nous dirigeons vers l’hiver de l’hémisphère nord. »
Il explique en détail comment et pourquoi les populations fortement vaccinées contre la COVID-19 vont : faire apparaître des variants toujours plus infectieux et potentiellement dangereux dérivées d’Omicron, par échappées immunitaire, tout en étant plus à risque de contracter une forme grave de COVID-19 que les populations moins ou non vaccinées.
Comment les risques d’autres affections chez les populations fortement vaccinées, y compris les cancers agressifs, précoces, les cancers « turbo » et les poussées auto-immunes, augmenteront probablement considérablement par rapport à ceux qui, prudents, choisissent d’éviter une injection supplémentaire contre la COVID-19.
La base de preuves pointant dans cette direction devient de plus en plus forte (avec de nombreuses références à d’autres publications dans le rapport de Vanden Bossche). »
La relation possible avec les cancers du sang et les vaccins COVID-19 et les mécanismes scientifiques avérés peuvent l’expliquer… mais l’essentiel est d’entendre que la hausse d’incidence des cancers depuis 2021 a moins d’une chance sur 1000 d’être due au hasard.
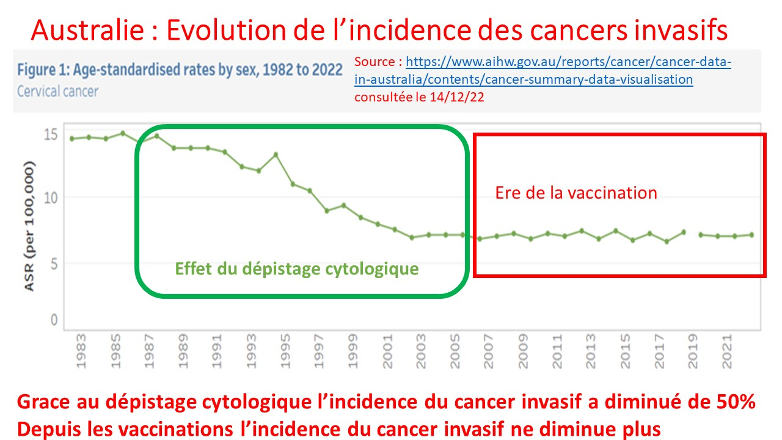
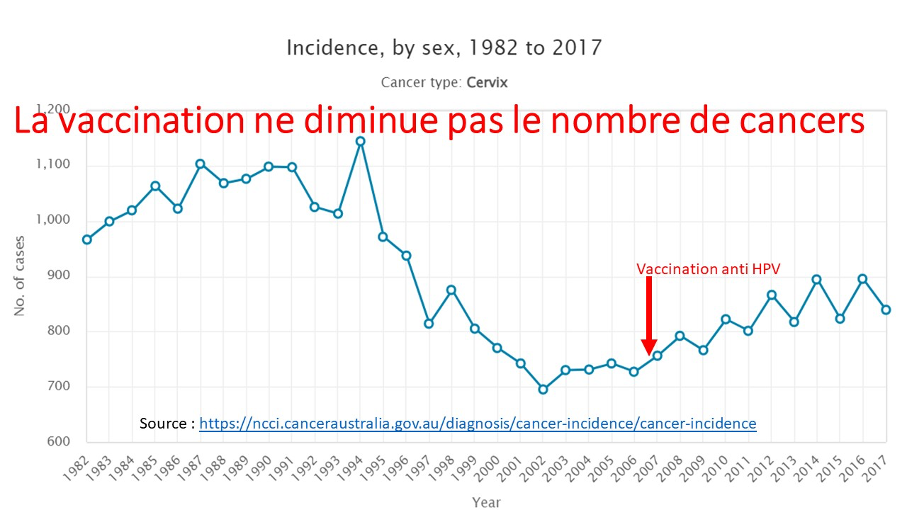
L’argument selon lequel l’épidémie de cancer serait due au retard dans les dépistages ne tient pas, car l’arrêt des dépistages et le retard aux traitements aboutissent à des formes plus évoluées de cancers et peut en augmenter la mortalité, mais est incapable d’en augmenter significativement l’incidence.
De plus si c’était le cas il s’agirait des cancers classiques. Or ici ce sont de nouveaux types de cancer, à des âges inhabituels avec des comportements particuliers tels leur vitesse majeure de développement et leur résistance à tous les traitements habituels.
« Nous voyons des cancers rares/bizarres et des augmentations hors saison. Les dépistages différés ne déclenchent pas une augmentation des cancers en une seule semaine. Il s’agit d’une intervention spécifique, intense et inédite ». As an Oncologist I Am Seeing People With Stable Cancer Rapidly Progress After Being Forced to Have a Booster », The Daily Sceptic
On comprend pourquoi les injections suivant la première sont plus toxiques :
« Lorsqu’il y a une stimulation du système immunitaire, la microglie ramifiée passe au stade de la microglie amorcée. Les pseudopodes sont rétractés et cela devient une cellule plus arrondie. À l’intérieur de la microglie amorcée, il y a une intense régulation à la hausse de la production de cytokines, de chimiokines et d’excitotoxines — mais elles ne sont pas libérées de la cellule, il peut donc y avoir une réaction immunitaire mineure, mais sinon il n’y a pas beaucoup de signes de réaction. C’est ce qui se passerait avec la première injection de cet injectable qu’ils appellent un ‘vaccin’ », a déclaré le Dr Blaylock.
Il est important de noter que les chimiokines attirent les macrophages, ou globules blancs, vers le cerveau. Un macrophage dans le cerveau ressemble exactement à la microglie et peut également subir un amorçage.
« Avec la deuxième stimulation immunitaire, [qui serait la deuxième injection et] qui peut être des mois plus tard, cette microglie amorcée devient complètement activée. Et lorsque cela se produit, il libère tous ces composants toxiques… vous obtenez une microglie activée de manière chronique, [un] état suractivé et il y a une réaction inflammatoire 3 fois plus élevée que celle que vous obtiendriez normalement avec l’activation microgliale. »
Le Dr Blaylock insiste sur les dangers sur les fœtus et les risques prévisibles à long terme :
« Je pense que comme conséquence des injections de Covid Nous allons assister à une augmentation considérable des troubles du spectre autistique. L’autre trouble dont on ne parle jamais est la schizophrénie. Ce que nous voyons, c’est que si nous stimulons le système immunitaire au cours du troisième trimestre, l’incidence de la schizophrénie augmente d’environ 6 fois. Mais ça n’arrive qu’à l’adolescence donc ça va être long avant qu’on le voie.
« Mais je pense que tout — les malformations augmentent déjà de 300 à 400 %, les fausses couches — nous allons voir des choses que nous n’avons jamais vues auparavant. C’est la tragédie de tout cela.
Que les organisations pédiatriques approuvent les injections de Covid est monstrueux. »
Le Dr Ryan Cole a remarqué qu’il y avait une augmentation considérable des cancers agressifs après le déploiement de l’injection de Covid. Il a également remarqué que les personnes qui avaient des cancers bien contrôlés développaient des cancers incontrôlables et mouraient très rapidement.
De longues publications abordent maintenant ce sujet. L’important en urgence est de stopper ces injections et de les éviter à vos proches en attendant une suppression mondiale.
« L’idée qu’un nouveau produit comme les vaccins [COVID] pourrait causer le cancer n’est pas quelque chose qui sera observable du jour au lendemain », a expliqué le Dr Risch dans une interview passionnante
« Le cancer en tant que maladie prend beaucoup de temps à se manifester à partir du moment où il commence, des premières cellules qui se détraquent jusqu’à ce qu’elles deviennent assez grandes pour être diagnostiquées ou symptomatiques, peut prendre de deux ou trois ans pour les cancers du sang, comme les leucémies et les lymphomes, à cinq ans pour le cancer du poumon. à 20 ans pour le cancer de la vessie, ou 30, 35 ans pour le cancer du côlon, et ainsi de suite.
« Ce sont donc des événements à long terme, et si vous introduisez soudainement un nouveau produit comme les vaccins, la première chose que vous pourriez vous attendre à voir serait les cancers du sang que j’ai mentionnés, mais pas les autres types de cancers. »
Les troubles liés au sang apparaissent déjà dans les données britanniques que nous avons signalées précédemment
Mais il ne s’agit pas seulement de troubles hématologiques
Les cancers qui prennent normalement dix, vingt ou trente ans à se développer, théoriquement accélérés par les vaccins immunosuppresseurs contre la COVID, pourraient apparaître à des taux accrus à long terme, a laissé entendre le Dr Risch.
Mais à moyen terme nous voyons déjà des signes de cela se produire alors que les jeunes, dans la fleur de l’âge, souffrent du cancer à des taux sans précédent.
Colby Brock, un YouTuber de 26 ans, a partagé son diagnostic de cancer des testicules avec ses abonnés le 9 juillet 2023. Le Dr William Makis a fait une plongée profonde dans les jeunes influenceurs des médias sociaux qui contractent le cancer sur sa page Substack.
Selon le Dr Risch, si une personne de 25 ans développe un cancer du côlon sans antécédents familiaux de la maladie, « c’est fondamentalement impossible selon le paradigme connu du fonctionnement du cancer du côlon ». Il a ajouté que d’autres cancers à longue latence font surface chez les très jeunes. « Ce n’est tout simplement pas l’occurrence normale du fonctionnement du cancer. »
« Parce que ces cancers se sont produits chez des personnes trop jeunes pour les avoir, par rapport à la façon normale de survenue, ils ont été désignés comme des turbo-cancers », a ajouté le Dr Risch.
« Certains de ces cancers sont si agressifs qu’entre le moment où ils sont vus pour la première fois et le moment où ils viennent pour le traitement après quelques semaines, ils ont considérablement augmenté par rapport à ce à quoi les oncologues s’attendaient. »
« Il doit y avoir un stimulus initiateur », a-t-il déclaré. Comme déjà mentionné, « les vaccins contre la COVID ont causé divers degrés de dommages au système immunitaire chez une fraction des personnes qui les ont pris. » « si vous endommagez le système immunitaire d’une manière qui limite la capacité de reconnaître ou de désactiver les cellules cancéreuses dérangées en croissance naissante, cela ouvre la porte à leur multiplication au point où il est au-delà du système immunitaire de faire face. Et c’est le mécanisme, je pense, qui est le plus probable ici. »
Des exemples se multiplient dans la littérature institutionnelle aussi bien que sur les réseaux sociaux citons cette observation à propos d’enseignants Makis
En conclusion
Il faut refuser tout nouveau booster car toutes les études montrent une augmentation extrême de certaines maladies associées au déploiement de l’inoculation de l’ARNm et l’inefficacité de ces injections à protéger du covid ceux qui les reçoivent.
En particulier, nous pouvons observer que les maladies hématologiques malignes ont connu une augmentation extraordinaire par rapport au début de 2021, presque coïncidant avec le déploiement du vaccin Covid-19.
Nous observons également l’augmentation des réclamations liées aux maladies cardiovasculaires et des réclamations liées au système musculo-squelettique, qui sont probablement dues à une inflammation. Nous observons également que l’augmentation des cancers a, jusqu’à présent, été modérée, mais nous sommes préoccupés par le fait que ces résultats sont de nature à plus long terme et devraient donc continuer à augmenter dans les années à venir.
Refusez le booster à ceux que vous aimez
Les appels internationaux à stopper cette catastrophe sanitaire sont nombreux. En décembre 22, nous diffusions cet appel à protéger vos proches, et qu’il est impératif de refaire à nouveau, devant la volonté du ministre de la Santé de reprendre les injections à partir du 2 octobre 23, en « favorisant les plus fragiles » en sachant (mais le sait-il ?) que ce sont ceux-là même qui sont le plus à risque de complications de l’injection-expérimentale.
Et les EHPAD vont continuer à se vider, les établissements privés ayant de plus en plus de difficultés à trouver des candidats pour les remplir…Si vous aimez vos proches injectés (par confiance mal placée aux médias menteurs, ou par nécessité vitale pour vivre), protégez-les du booster proposé, car les effets s’accumulent avec les doses successives, d’autant que le contenu de ces nouveaux pseudovax paraît de plus en plus riche en substances toxiques. Les premières doses contenaient beaucoup de placebos, mais les suivantes sont de plus en plus riches en ARNm et en graphène, d’ou une multiplication des complications que chacun peut constater dans son entourage s’il ne se voile pas la face.
Alors si vous tenez à vos proches et amis, informez -les pour qu’ils sachent à quoi ils s’exposent.
https://www.humanite.fr/en-debat/covid-19/grand-entretien-avec-axel-kahn-contre-le-covid-19-une-couverture-vaccinale-de-60-ferait-la-difference-697120
https://perma.cc/2D5K-G694
Les apprentis sorciers éditions Albin Michel – paru le 8 mars 2023
Les cancers augmentent considérablement en tandem avec les vaccinations Covid (2ndsmartestguyintheworld.com) Vanden Bossche envoie un avertissement sévère à ceux qui envisagent de se faire vacciner contre la COVID-19 plus tard cette année, alors que nous nous dirigeons vers l’hiver de l’hémisphère nord.
Il explique en détail comment et pourquoi les populations fortement vaccinées contre la COVID-19 :
Servir à conduire des variantes toujours plus infectieuses et potentiellement dangereuses, échappées immunitaires, dérivées d’Omicron.
Être plus à risque de contracter une forme grave de COVID-19 que les populations moins vaccinées ou non vaccinées.
Comment le risque d’autres affections chez les populations fortement vaccinées, y compris les cancers agressifs, précoces, les cancers « turbo » et les poussées auto-immunes, augmentera probablement considérablement par rapport à ceux qui choisissent d’éviter une vaccination supplémentaire contre la COVID-19.
L’arnaque du dépistage du cancer de la prostate – Docteur Nicole Delépine (nicoledelepine.fr)
Un article français à lire absolument si on désire subir le dépistage organisé du cancer du sein – Docteur Nicole Delépine (nicoledelepine.fr)
https://childrenshealthdefense.org/defender/dr-ryan-cole-shots-hooker/
Ref in ibid 5 https://t.me/alexandrahenrioncaude
Naissance : https://calgaryherald.com/calgary-zoos-baby-gorilla-finally-has-a-name
Antécédents : https://calgaryherald.com/zoos-gentle-giant-gorilla-kakinga-dead-at-37
Injection : https://globalnews.ca/calgary-zoo-animals-first-dose-covid-19-vaccine
Soin palliatif comme seule solution : https://www.cbc.ca/gorilla-kimani-calgary-zoo-cancer
Angus Dalgleish Rapid Response:Re: Covid-19: Fourth vaccine doses—who needs them and why? BMJ 2022; 376 doi: https://doi.org/10.1136/bmj.o30 (Published 07 January 2022) Cite this as: BMJ 2022;376:o30
https://www.linkedin.com/pulse/inescapable-immune-escape-pandemic-geert-vanden-bossche?trk=public_post
Geert Vanden Bossche, Robert Rennebohm The Inescapable Immune Escape Pandemic Kindle Edition
Dr Russell Blaylock : Comment les protéines de pointe induites par les vaccins endommagent le cerveau et causent le cancer, par Rhoda Wilson 22 novembre 2022
L’interview complète du Dr Risch avec The Epoch Times est disponible via le lien ci-dessous:
Dr Harvey Risch: Augmentation des « cancers turbo » agressifs – et en particulier chez les jeunes
septembre 2023
TURBO CANCER – Les enseignants sont décimés par des cancers agressifs et métastatiques après les obligations de vaccin à ARNm COVID-19 – 34 cas tragiques récents aux États-Unis! (substack.com) 6 SEPT. 2023
Makismd.substack.com/p/turbo-cancer- teachers- are- being- decimated
Royaume-Uni – Analyse PIP – Systèmes de carrosserie (phinancetechnologies.com)
Flambée de cancers sous pseudovax : conseils aux naïfs tentés par un nième booster – Profession Gendarme (profession-gendarme.com)
Alliance for Natural Health International initialement et Children’s Health Defense
www.anhinternational.org/news/feature-the-scientific-case-for-an-immediate-halt-to-covid-vaccination-of-children